-
 Scleral Indentation In A Normal Eye
Scleral Indentation In A Normal Eye
Nov 9 2012 by Norman Byer
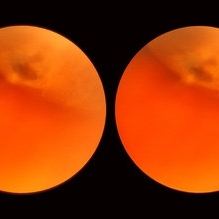
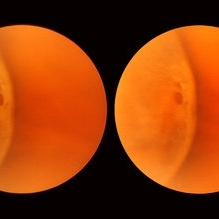
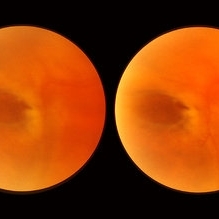
This shows the appearance of scleral indentation in a normal eye. Note the convex shadow which marks the posterior border of the indented area. It is caused in part by a small angle which separates the viewing axis from the illuminating axis thus allowing the observer to see slightly into the shadow beyond the illuminated crest of the indentation. It is also caused in part by viewing the pigment epithelial layer in a tangential manner. This shadow is of great diagnostic usefulness since it becomes a dark background against which many tiny retinal abnormalities can be seen beautifully by contrast. Two other particular advantages of scleral indentation will be demonstrated in the following photographs: First, the ability to see the extreme anterior part of the retina to the ora serrata and beyond, and second, the ability to examine any abnormality in multiple profiles depending on slight movements of the scleral depressor in various directions.
Condition/keywords: extreme anterior retina, posterior border, scleral indentation, shadow, tangential view of pigment epithelial layer
-
 Normal Temporal Ora Serrata
Normal Temporal Ora Serrata
Nov 9 2012 by Norman Byer
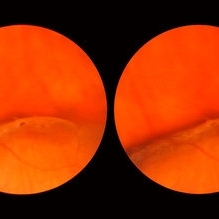
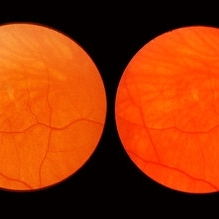
This is the normal temporal ora serrata in a 26-year-old man. Note the typical ragged moth-eaten appearance caused by peripheral cystoid degeneration. This appearance may be present in infants but is always present beyond the age of eight years.
Condition/keywords: ora serrata, peripheral cystoid degeneration
-
 Normal Nasal Ora Serrata
Normal Nasal Ora Serrata
Nov 9 2012 by Norman Byer
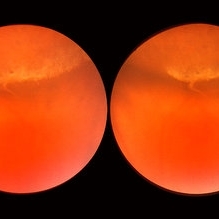
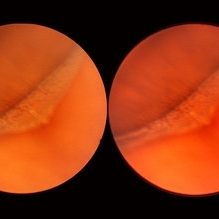
This shows the normal nasal ora serrata. Note the dentate processes which divide the nasal ora into prominent bays and teeth
Condition/keywords: dentate processes, normal nasal ora serrata, ora bay, ora teeth
-
 Normal Nasal Ora Serrata
Normal Nasal Ora Serrata
Nov 9 2012 by Norman Byer
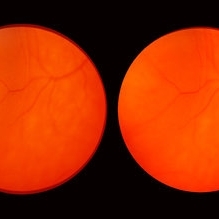
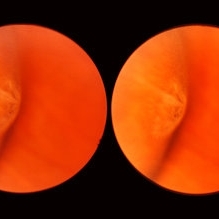
This is the normal nasal ora serrata showing a prominent meridional fold. Such folds are most commonly seen at the lower part of the upper nasal quadrant, and are present in 26% of the population. They are a normal developmental variation and are often bilateral.
Condition/keywords: meridional fold, normal developmental variation, normal nasal ora serrata, upper nasal quadrant
-
 Enclosed Ora Bay On The Temporal Side
Enclosed Ora Bay On The Temporal Side
Nov 9 2012 by Norman Byer
This is a developmental abnormality in a 59-year-old man. It is an enclosed ora bay on the temporal side, an isolated island of normal pars plana epithelium. It is important not to confuse this entity with a retinal break. It has smooth, sloping borders not a sharp, thin, visible retinal edge as a retinal break would have. The border looks exactly like that of the ora serrata, and the grayish pigmented base has the same appearance as the normal pars plana.
Condition/keywords: developmental abnormality, enclosed ora bay, grayish pigmented base, horizontal nasal meridian, pars plana epithelium, smooth sloping borders, temporal retina
-
 Enclosed Ora Bay On The Temporal Side
Enclosed Ora Bay On The Temporal Side
Nov 9 2012 by Norman Byer
This is another example of an enclosed ora bay on the temporal side. It is surrounded by normal retina and well separated from the ora serrata, which is toward the upper right just beyond the photograph. The yellow nubbin marks an abortive dentate process.
Condition/keywords: abortive dentate process, enclosed ora bay, normal eye, normal retina, ora serrata, temporal retina
-
 Peripheral Retinal Lesion
Peripheral Retinal Lesion
Nov 9 2012 by Norman Byer
This small elevated peripheral retinal lesion in a 48-year-old woman is a cystic retinal tuft. Such tufts are congenital developmental anomalies present from birth and situated behind the vitreous base. They are sites of abnormal vitreoretinal attachment, and can occasionally lead to retinal tears at the time of posterior vitreous detachment. They are present in about 5% of patients.
Condition/keywords: abnormal vitreal retinal attachment, behind the vitreous base, congenital anomaly, cystic retinal tuft, developmental anomaly, peripheral retinal lesion, present from birth
-
 Asymptomatic Lesion
Asymptomatic Lesion
Nov 9 2012 by Norman Byer
This asymptomatic lesion in a 27-year-old woman is a very interesting example of a cystic retinal tuft. Note the discrete white nubbin, which is the chief characteristic of this lesion. In this case, it is surrounded by a small area of subretinal fluid. The next slide pair will reveal the reason for this.
Condition/keywords: asymptomatic, cystic retinal tuft, subretinal fluid
-
 Asymptomatic Lesion
Asymptomatic Lesion
Nov 9 2012 by Norman Byer
This is the same lesion as seen in the previous slide pair. Here the scleral indentation is carried more posterior revealing a tiny, round, full thickness retinal hole. This is not a tear produced by traction even though vitreous is always attached to these flaps. You will note that the hole is round and is separated by a slight distance from the flap itself. It is probably the result of long continued atrophy and devitalization of the retina. A posterior vitreous was not detached. This lesion has not changed its appearance for more than a year of observation, but the age of the hole is actually unknown.
Condition/keywords: asymptomatic, atrophy, full thickness retinal hole, posterior scleral indentation, retinal hole, round hole
-
 White Retinal Tuft
White Retinal Tuft
Nov 9 2012 by Norman Byer
This white retinal tuft was seen in a 20-year-old man. It is associated with an asymptomatic retinal tear posterior to the tuft and with a tiny adjacent amount of subretinal fluid. It remained just like this for six years and then underwent the change shown in the next slide pair.
Condition/keywords: asymptomatic, subretinal fluid, white retinal tuft
-
 White Retinal Tuft
White Retinal Tuft
Nov 9 2012 by Norman Byer
After six years, the previous lesion looked like this. The former flap has been completely avulsed and is now a free operculum. The white zone around the tear represents the small area of detachment and subretinal fluid. It is still asymptomatic and does not require treatment.
Condition/keywords: does not require treatment, free operculum, operculated retinal hole, subretinal fluid, white retinal tuft
-
 White Retinal Tuft
White Retinal Tuft
Nov 9 2012 by Norman Byer
This is the fellow eye of the previous patient showing three tiny delicate tufts with parts of the tufts avulsed by vitreous traction. These lesions are symmetrically located in the fellow eye as compared to the lesion in the previous two slides.
Condition/keywords: symmetrical, vitreous traction, white retinal tuft
-
 Sudden Posterior Vitreous Detachment
Sudden Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
This 60-year-old man suffered a sudden posterior vitreous detachment which produced a large tractional retinal tear at 11:30 o’clock in this eye. This white cystic retinal tuft located at 9:30 also suffered minor injury at the same time as revealed in the next slide pair.
Condition/keywords: posterior vitreous detachment, white retinal tuft
-
 Sudden Posterior Vitreous Detachment
Sudden Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
This is the same lesion seen in the previous slide pair. With the scleral indentation performed more posteriorly, a small hemorrhage can be seen on the white tuft. This is proof of the vitreal retinal attachment at this spot. Posterior vitreous detachment can produce a retinal tear at the site of a cystic retinal tuft, but in this case has caused only a small hemorrhage.
Condition/keywords: posterior vitreous detachment, retinal hemorrhage, scleral indentation, vitreoretinal attachment
-
 Sudden Posterior Vitreous Detachment
Sudden Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
This 52-year-old woman suffered a sudden posterior vitreous detachment which caused a large horseshoe tear at 12:00 o’clock in this eye. It also produced another change at 8:45 in this left eye shown in this photograph. Note the small hemorrhage just to the left of the vessel. Immediately to the left of the hemorrhage and lying alongside of the vessel is a yellowish lesion which actually represents a cystic retinal tuft. You will see it better in the next slide pair.
Condition/keywords: cystic retinal tuft, posterior vitreous detachment, retinal hemorrhage, retinal vessel
-
 Sudden Posterior Vitreous Detachment
Sudden Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
In this view of the previous case, the scleral indentation is being done immediately beneath the lesion. The hemorrhage is now out of sight and the white lesion is seen to be distinctly he elevated and in two parts. The base is white and the apex is translucent with a possible small hole in it. There is also a probable tiny full- thickness tear just behind the flap which cannot be discerned in this view.
Condition/keywords: full thickness retinal tear, peripheral retinal lesion, scleral indentation, translucency of apex, white retinal lesion
-
 Sudden Posterior Vitreous Detachment
Sudden Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
This is the same eye that was described in slide pairs 15 and 16 and shows a large tractional symptomatic retinal tear at 12 o’clock. It was caused by a posterior vitreous detachment which placed sudden traction on a cystic retinal tuft. The whitish tuft is barely visible on the flap because it is not in focus. This tear was treated successfully with cryotherapy. The next slide pair is a postoperative view of the same lesion.
Condition/keywords: cystic retinal tuft, posterior vitreous detachment, tractional retinal tear
-
 Sudden Posterior Vitreous Detachment
Sudden Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
This is the appearance of the previous lesion three weeks following prophylactic cryotherapy. Continuing vitreal retinal traction has a now torn the flap completely free from the retina. The whitish cystic retinal tuft can be discerned on the upper part of the free operculum. Along the lower half of the operculum superimposed over the dark shadow of the scleral indentation one may observe numerous, delicate, vitreous fibrils actually attaching to the operculum.
Condition/keywords: cystic retinal tuft, free operculum, prophylactic cyrotherapy, retinal flap, scleral indentation, vitreoretinal traction, vitreous fibrils
-
 Cystic Retinal Tuft
Cystic Retinal Tuft
Nov 9 2012 by Norman Byer
This is a rather poor photograph taken in 1969 but is important for comparison with the next slide pair. It shows a cystic retinal tuft in a 49-year-old woman and was taken without scleral indentation. The two pigment spots just inferior to the tuft represent a secondary degenerative change in the pigment epithelium.
Condition/keywords: cystic retinal tuft, degenerative changes of retinal pigment epithelium, pigmented spots
-
 Cystic Retinal Tuft
Cystic Retinal Tuft
Nov 9 2012 by Norman Byer
This is the same lesion as in the previous slide pair but the photograph was taken nine years later when the patient was 58-years-old soon after an acute posterior vitreous detachment. This demonstrates that posterior vitreous detachment can produce large retinal tears at these sites. However, it is important to emphasize that prophylactic treatment of cystic retinal tufts in the absence of a retinal tear would be very ill-advised because several hundred innocence and harmless lesions would have to be treated in order to prevent one tear of the retina.
Condition/keywords: cystic retinal tuft, posterior vitreous detachment, retinal tear
-
 Posterior Vitreous Detachment
Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
This 68-year-old woman had a recent posterior vitreous detachment which produced this symptomatic horseshoe tear exactly at the site of this cystic retinal tuft. Note the characteristic discrete white nubbin at the apex, which is produced by a cap of glial cells with densely packed cytoplasm.
Condition/keywords: cystic retinal tuft, glial cells, posterior vitreous detachment, white retinal tuft
-
 Symptomatic Retinal Tear
Symptomatic Retinal Tear
Nov 9 2012 by Norman Byer
This is another example of a symptomatic retinal tear which occurred at the site of a cystic retinal tuft two days prior to the photograph when an acute posterior vitreous detachment occurred in this 64-year-old woman. Note the horizontal line of vitreous blood along the lower edge of the flap which demarcates the vitreous attachment to the flap.
Condition/keywords: acute posterior vitreous detachment, cystic retinal tuft, retinal flap, retinal tear, vitreous blood
-
 Symptomatic Horseshoe Tear
Symptomatic Horseshoe Tear
Nov 9 2012 by Norman Byer
This is a fresh, symptomatic horseshoe tear at the site of a cystic retinal tuft in a 63-year-old man. This is really a double horseshoe tear because the two retinal vessels have resisted the vitreal retinal traction and have preserved an intact bridge of tissue between the tears. Note the prominent vitreous condensation attached to the apex of the upper tear and made much more visible because it is seen superimposed over the dark underlying shadow of scleral indentation.
Condition/keywords: bridge of tissue between tears, cystic retinal tuft, scleral indentation, vitreous condensation
-
 Vitreous Hemorrhage
Vitreous Hemorrhage
Nov 9 2012 by Norman Byer
This 60-year-old man suddenly developed a vitreous hemorrhage from this acute horseshoe tear 3½ years following cataract extraction when a posterior vitreous detachment occurred. The white nubbin identifies this lesion as a preexisting cystic retinal tuft. The pigment spot beneath the flap is evidence of secondary trophic changes in the pigment epithelium. Note the irregular shape of the flap with the narrow tip and broad base. This was caused by vitreous traction which was exerted at two separate points on the retina and which tore the retina at each place.
Condition/keywords: acute posterior vitreous detachment, irregularly shaped flap, trophic pigmented changes, vitreous hemorrhage, vitreous traction, white retinal tuft
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
This is a very subtle example of lattice degeneration showing the mildest possible changes in a 27-year-old man. In the upper left there is a vein directed toward the center of the slide. Just above and to the right of the pigment spot it veers to the right and then abruptly disappears as it passes through the lattice lesion. As it leaves the lesion, it resumes its normal appearance going down to the right. In a similar manner, the arteriole in the lower left enters the lesion just to the right of the pigment spot, then disappears as it passes through the lesion and reappears later as it emerges. The only change in this lesion in 12 years was the appearance of the pigment spot.
Condition/keywords: lattice degeneration
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
This is a more typical classical example of lattice degeneration in a 42-year-old woman in a photograph taken without scleral indentation. It shows much more marked vascular changes than the previous case. Note the tapering of the blood columns as the vessels approach the lesion and also the white sheathing of the vessel walls. Note also the continuity of the blood vessels on opposite sides of the lesion with the characteristic white lattice lines. More than 45 years ago Vogt pointed this out as a proof that these white lines were actually caused by changed blood vessels. Note also that this lesion shows a combination of several individual features of lattice degeneration. In addition to the white lines, there is a reddish crater-like area beneath the main horizontal white line. There is a prominent horizontal zone below this white line showing a snailtrack appearance. Also, there are two tiny atrophic retinal holes outside the photograph on the right end of this lesion. This eye contained five such retinal holes and they have all remained unchanged for more than 10 years of observation without treatment.
Condition/keywords: atrophic retinal hole, lattice degeneration, moderate snail track, tapering blood columns, white lattice lines, white sheath vessel
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
This is lattice degeneration in a 10-year-old boy showing an almost pure snailtrack feature with only a hint of a reddish crater in the center. It has not changed over 10 years. The photograph was taken with scleral indentation.
Condition/keywords: lattice degeneration, reddish crater, scleral indentation, snail track
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 36-year-old woman has remained unchanged over a period of 13 years. It shows a moderate snailtrack feature with discrete yellow dots visible on the surface of the lesion and especially along the posterior border. One of these can be well seen just below the lesion superimposed over the dark shadow of the scleral indentation. The exact nature of these yellow dots is still not entirely clear.
Condition/keywords: lattice degeneration, moderate snail track, scleral indentation, yellow dots
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 27-year-old woman shows an interesting change in the middle of the lesion. The predominant feature on the left side of the lesion is the snailtrack appearance while the right side of the lesion shows mainly a reddish crater. Note the many yellow dots above the surface of the retina which are actually located in the vitreous condensation which surrounds the pocket of liquified vitreous over the lesion.
Condition/keywords: lattice lesion, reddish crater, snail track, vitreous condensation, vitreous liquefaction
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 30- year-old woman also shows combined features with a reddish crater above and a parallel snailtrack appearance just below it. Please note especially another interesting feature. From the left end of the lesion, there is a faint thin yellow line slanting down toward the right just below the shadow of the scleral indentation. This line identifies the dome of the pocket of liquified vitreous which is present over every lesion of lattice degeneration.
Condition/keywords: lattice degeneration, lattice lesion, liquefied vitreous, reddish crater, scleral indentation, snail track
-
 Parallel Lattice Lesions
Parallel Lattice Lesions
Nov 9 2012 by Norman Byer
This is an example of parallel lattice lesions. The anterior one is faintly seen and not in focus. The posterior lesion shows a prominent whitish meshwork with modeled reddish areas which sometimes may be mistaken for retinal holes.
Condition/keywords: lattice degeneration, lattice lesion, parallel lattice lesions, reddish areas, scleral indentation
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 27-year-old woman shows a reddish crater with much pigmentation. The pigment clumping is caused by a secondary degenerative change in the pigment epithelium. An arteriole crosses the upper end of the lesion and it becomes very narrow and its walls become white has it does so.
Condition/keywords: degenerative changes of retinal pigment epithelium, lattice degeneration, lattice lesion, pigment clumps, pigment epithelium, reddish crater, secondary degenerative change
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 70-year-old woman is almost entirely pigmented but several white lines can be faintly seen.
Condition/keywords: lattice degeneration, lattice lesion, pigmented lattice lesion, white lattice lines
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in an 18-year-old girl shows the combination of a reddish crater, several prominent pigment clumps and white lines. Please note that the white vessel changes involve both arterioles and venules.
Condition/keywords: lattice degeneration, lattice lesion, pigment clumps, reddish crater, white lattice lines
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
This lesion in a 51-year-old woman is also an example of lattice degeneration but shows only a uniform reddish crater with no other features. This lesion has remained exactly the same for 9 years but such red craters sometimes give rise to punched-out atrophic retinal holes which may lead to subclinical retinal detachment. This sequence of events will be shown in the next two slide pairs.
Condition/keywords: lattice degeneration, lattice lesion, reddish crater
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This is a photograph of a lattice lesion in a 23-year-old girl taken without scleral indentation. Just to the left of the center of the slide is a slightly pigmented lesion almost oval in shape with a retinal hole in each end. Ten years earlier at the age of 13 this lesion appeared exactly like the one in the previous case as a pure red crater. Five years later two new round retinal holes were seen, one in each end, with a tiny bit of subretinal fluid within the lattice lesion only. Five years later still the appearance was as shown in this slide pair with the subretinal fluid now extending slightly beyond the lattice lesion as far as the curved row of tiny yellow exudates seen just to the right of the center of the slide. It is now actually a small subclinical retinal detachment. The next slide pair will show this better using scleral indentation.
Condition/keywords: lattice degeneration, lattice lesion, pigmented lesion, reddish crater, retinal hole, subretinal fluid, yellow exudate
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This is the same lesion as seen in the previous case seen now with scleral indentation. Here you can see directly into the subretinal space through the two retinal holes. The holes appear dark because the shadow of the scleral indentation lies directly beneath them.
Condition/keywords: lattice degeneration, retinal hole, scleral indentation
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 21-year-old woman shows an interesting white with pressure configuration to the upper left of the dark lesion. This whitish area is of no clinical importance.
Condition/keywords: lattice degeneration, white with pressure
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 44-year-old woman shows an interesting tuft arising from the edge of the lesion and seen well against the background of the shadow of the indentation. It is caused by glial proliferation into the vitreous condensation at the edge of the lesion. Around the borders of each lattice lesion there is an invariable attachment of condensed vitreous. It is this vitreoretinal attachment that comprises the chief danger of lattice lesions where it may lead to acute retinal tears and retinal detachment at the time of posterior vitreous detachment.
Condition/keywords: glial proliferation, lattice degeneration, scleral indentation, vitreoretinal attachment, vitreous condensation, white retinal tuft
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 44-year-old man shows an atrophic retinal hole surrounded by discrete yellowish and pigmented areas. These have been caused by secondary pigment migration and proliferation in the retinal pigment epithelium. There is a small doughnut like elevation of the retina between the edge of the hole and the line of pigment. The lesion and the hole have remained exactly the same for seven years.
Condition/keywords: atrophic retinal hole, elevated retina, lattice degeneration, lattice lesion, proliferation of retinal pigment epithelium, scleral indentation
-
 Flat Lattice Lesion
Flat Lattice Lesion
Nov 9 2012 by Norman Byer
This 34 year-old man had a flat lattice lesion with no hole at this location for five years. Then he developed this round hole with a small subclinical retinal detachment which has not changed in appearance for four years. Note the tiny glial tuft just to the left of the hole and superimposed against the dark background.
Condition/keywords: glial tuft, lattice degeneration, round hole
-
 Lattice Combined with Tiny Round Hole
Lattice Combined with Tiny Round Hole
Nov 9 2012 by Norman Byer
This 45 year-old man shows the snail track form of lattice combined with a tiny round hole. There is a tiny subclinical retinal detachment confined to the lesion itself.
Condition/keywords: glial vitreous tuft, lattice degeneration, round hole, snail track
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
When this boy was first examined at the age of six years, he had only the red crater form of lattice at this location. This photograph shows the same lesion at age 11 and there is now a small round atrophic hole with a tiny round zone of detachment around it. It has not changed for four years.
Condition/keywords: atrophic retinal hole, lattice degeneration, lattice lesion, reddish crater, round hole
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 44-year-old woman shows combined features of pigmentation, white lines, yellow dots and a round hole with a tiny zone of adjacent detachment. There are three such holes in this eye and they have not changed or been treated for eight years.
Condition/keywords: adjacent detachment, atrophic retinal hole, lattice degeneration, lattice lesion, pigmented lattice lesion, round hole, white lattice lines, yellow dots
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
This 16-year-old girl has lattice degeneration and also this large oval retinal hole with a surrounding narrow zone of subretinal fluid. This lesion illustrates how large the atrophic holes of lattice degeneration may be. Occasionally the hole can be as large as the initial lattice lesion and can therefore obliterate all other evidence of its true identity. This was almost true in this case, but there does remain a small whitish remnant of the original lattice lesion at the lower end of the oval hole.
Condition/keywords: lattice degeneration, retinal hole, subretinal fluid, white lattice lines
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
Lattice lesion that was originally just a reddish crater as in slide pair 35 in a girl 14 years of age. By the time she was 21, seven years later, it had changed to this appearance, more whitish and with a tiny hole in the right end. This hole has led to a small subclinical retinal detachment which extends beyond the lattice lesion to the margin of the yellow zone. It has remained exactly like this for more than 21 years.
Condition/keywords: lattice degeneration, lattice lesion, retinal hole
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This lattice lesion in a 36-year-old woman shows a snail track feature on the left combined with a reddish crater and retinal hole to the right. The hole has caused a small subclinical detachment. The next slide pair will show more of this lesion.
Condition/keywords: lattice lesion, reddish crater, retinal hole, snail track, subclinical detachment
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This is the same lesion as shown in the previous case. Two retinal holes are present, and you can look through the upper hole into the dark subretinal space. This is, therefore, a true subclinical retinal detachment but it has changed only slightly in the past 13 years. About 75% of such holes in lattice lesions show a tiny adjacent zone of subretinal fluid. After the hole forms from gradual progressive thing of the retina, a tiny amount of fluid from the pocket of liquified vitreous over the lesion passes through the hole to the subretinal space
Condition/keywords: lattice degeneration, liquefied vitreous, retinal hole, subretinal fluid
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
In this 47-year-old woman, this lattice lesion with a small hole in the right end has led to a subclinical retinal detachment which extends to the margin of the subtle yellowish zone almost at the upper edge of the photograph. This patient did not desire surgery, and the area of detachment has changed only a small amount in the past eight years. The risk of a clinical retinal detachment developing from lattice degeneration is less than 1 percent. In those cases where it does though, about 3 quarters are caused by a tractional tear and about one quarter are caused by an atrophic hole as in this case.
Condition/keywords: atrophic retinal hole, lattice degeneration, lattice lesion, retinal hole, yellowish zone
-
 Flat Lattice Lesion
Flat Lattice Lesion
Nov 9 2012 by Norman Byer
This 24-year-old woman had a flat lattice lesion without holes observed with no change for six years. She then developed two tiny retinal holes in this lesion and three years later the clinical retinal detachment shown here. She responded well to surgery. Even though such atrophic holes and lattice lesions may occasionally lead to a clinical detachment, it is important to understand that the mere presence of such holes is not an indication for prophylactic treatment. The reason for this is that we now know statistically that fewer than 1 percent of such cases lead to a retinal detachment.
Condition/keywords: lattice degeneration, retinal hole, scleral depression
-
 Atrophic Holes in Lattice Lesion
Atrophic Holes in Lattice Lesion
Nov 9 2012 by Norman Byer
In this 26-year-old woman, these two atrophic holes in a lattice lesion led to a clinical retinal detachment which was operated on successfully. In retinal detachments of this type resulting from non tractional atrophic holes, it has been found that 50% occur before the age of 30 years.
Condition/keywords: atrophic retinal hole, lattice lesion
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
In this 54-year-old woman, lattice degeneration has led to a large horseshoe tractional tear around the posterior side on one end of the lesion resulting in a clinical retinal detachment. Note the very attenuated blood column passing through the white sheath vessel that crosses the tear. This demonstrates that the white blood vessels and a fragment of attached tissue are the only structures which have escaped the tearing effect of the strong vitreoretinal traction which occurred. This usually is true, although, in some cases this bridging vessel may bleed.
Condition/keywords: bridging vessel, lattice degeneration, tractional retinal tear, white sheath vessel
-
 Retinal Tear in Aphakic Fellow Eye
Retinal Tear in Aphakic Fellow Eye
Nov 9 2012 by Norman Byer
This 59-year-old man presented with sudden symptoms of retinal detachment in his opposite aphakic eye secondary to a tiny retinal tear about 1/8th disc diameter in size. During the examination, the fellow eye shown here was found to have this much larger tractional tear approximately 2 disc diameters in total length. If you look carefully, you will see that this is really a series of three separate tears with a common flap. The tears are separated by tiny bridges of remaining tissue which cause the edges of the apparent large tear to be serrated. This was also an aphakic eye with a posterior vitreous detachment but the lesion had produced no symptoms.
Condition/keywords: asymptomatic, bridge of tissue between tears, posterior vitreous detachment, tractional retinal tear
-
 Acute Retinal Detachment
Acute Retinal Detachment
Nov 9 2012 by Norman Byer
This 54-year-old man was referred because of sudden symptoms in his opposite eye in which he had suffered an acute retinal detachment secondary to a horseshoe tear around lattice degeneration. During the examination, the fellow eye shown here was also found to have this large horseshoe tear about 1 o’clock hour (4 disc diameters) in size. A tear occurred around a lattice lesion which is present on the flap but is out of focus. This tear had been asymptomatic even though it was caused by a posterior vitreous detachment and illustrates that even very large tears may produce no symptoms or mild symptoms that are easily overlooked.
Condition/keywords: lattice degeneration, posterior vitreous detachment
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
Lattice degeneration in a 42-year-old man which has produced four atrophic holes in a linear arrangement surrounded by a subclinical retinal detachment of unknown duration. By age 63, 21 years later, a posterior vitreous detachment was diagnosed in this eye, which was not present four years earlier. Nevertheless, the appearance seen here has remained exactly the same for 30 years, more than eight years with a concurrent PVD.
Condition/keywords: atrophic retinal hole, lattice degeneration, posterior vitreous detachment
-
 Lattice Degeneration
Lattice Degeneration
Nov 9 2012 by Norman Byer
Lesion immediately adjacent to the ora serrata in an 18-year-old boy probably represents lattice degeneration characterized primarily by a reddish crater. It has remained unchanged for more than three years.
Condition/keywords: lattice degeneration, ora serrata, reddish crater
-
 Asymptomatic Tractional Tear
Asymptomatic Tractional Tear
Nov 9 2012 by Norman Byer
This 38-year-old man was found to have this asymptomatic tractional tear in which the vitreoretinal traction had completely avulsed this tiny fragment of retina as a free operculum. Note how the examination and also the photography of this tiny lesion is made easier by scleral indentation.
Condition/keywords: asymptomatic, free operculum, scleral indentation, vitreoretinal traction
-
 Retinal Break
Retinal Break
Nov 9 2012 by Norman Byer
This is the right eye of a 49-year-old woman showing a tiny retinal break adjacent to the temporal ora serrata. It has remained exactly the same without treatment for nine years.
Condition/keywords: ora serrata, retinal break
-
 Posterior Vitreous Detachment
Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
In this 50-year-old man, these two adjacent tears are separated by a narrow band of tissue but have a common flap. They were caused by a posterior vitreous detachment and they are surrounded by a localized area of detachment. This case is similar to slide pair 53.
Condition/keywords: acute posterior vitreous detachment, adjacent tears, bridge of tissue between tears, posterior vitreous detachment, retinal tear
-
 Elevated Lesion
Elevated Lesion
Nov 9 2012 by Norman Byer
This photograph and the next are two views of a very interesting elevated lesion in a 45-year-old man. This photograph shows the immense value of closely scrutinizing the profile of the indented area. Note that in the middle of the slide there is a sudden break in the continuity of the dark convex shadow that lies just behind the crest of the scleral indentation. If the elevated tissue is "filmy" or "wispy" or filamentous as in this case, it raises a strong suspicion that a retinal break is present just behind it.
Condition/keywords: elevated retinal lesion, elevated tissue, retinal break, scleral indentation
-
 Elevated Lesion
Elevated Lesion
Nov 9 2012 by Norman Byer
This is the same case as the previous photograph. When the indentation is moved slightly more posterior, a small retinal tear is seen immediately behind the flap. Even though this is a true tractional tear, no retinal detachment has occurred over a period of 11 years of observation without treatment.
Condition/keywords: elevated retinal lesion, retinal tear, tractional retinal tear
-
 Aphakic Retinal Detachment
Aphakic Retinal Detachment
Nov 9 2012 by Norman Byer
This is an aphakic retinal detachment in a 66-year-old woman. Note the prominent yellow line which probably represents the posterior border of the vitreous base. Near the left end of the line there is a small retinal flap. At the exact location of this flap, there is a sudden break in the continuity of the yellow line, which is an important clue in finding this retinal tear. Often in aphakic detachments the causative tear is smaller than the one shown here and can be identified only by seeing a filamentous strand interrupting the uniform yellow line of the vitreous base.
Condition/keywords: aphakic retinal detachment, retinal flap, small retinal flap, vitreous base
-
 Retinal Detachment
Retinal Detachment
Nov 9 2012 by Norman Byer
This is a retinal detachment in a 55-year-old man. The vertical convex line on the right side probably represents the posterior border of the vitreous base. Note the small tractional tear with the base of its flap attached at this line. This demonstrates how the vitreous base presents an effective barrier to further extension of the retinal tear. Note also how the flap breaks the continuity of the yellow line.
Condition/keywords: retinal degeneration, retinal flap, tractional retinal tear, vitreous base
-
 Aphakic Retinal Detachment
Aphakic Retinal Detachment
Nov 9 2012 by Norman Byer
This 75-year-old woman had a scleral buckling operation on this aphakic eye two months previously. Two months following surgery she again had new symptoms of blurred vision and was found to have a redetachment caused by this small tractional retinal tear which may have been missed at the time of her original operation.
Condition/keywords: aphakic eye, scleral buckle, tractional retinal tear
-
 Horseshoe Tear
Horseshoe Tear
Nov 9 2012 by Norman Byer
This horseshoe tear was the cause of the detachment in this 54-year-old man. The orange area on the right half of the slide represents the area of scleral indentation. Please note that most of the tear lies over the indented area and appears orange. However, the extreme left side of the tear is brownish black in color because it is exactly superimposed over the dark shadow that always lies just beyond the indented area. The ability of scleral indentation to produce this color change combined with a sharp demarcation between the blackish area and the yellowish edge of intact retina is a pathognomonic sign of a full thickness retinal break.
Condition/keywords: scleral indentation
-
 Retinal Detachment
Retinal Detachment
Nov 9 2012 by Norman Byer
The retinal detachment in this 52-year-old man was brought on by this oval tear which has no flap or free operculum. This is however still a tractional tear caused by the retina pulling away from a corneoretinal adhesion, which is marked by the yellow spots seen through the tear. Actually, therefore, the operculum is behind the retina and attached to the pigment epithelial layer.
Condition/keywords: corneoretinal adhesion, operculum, tractional retinal tear
-
 Retinal Detachment
Retinal Detachment
Nov 9 2012 by Norman Byer
This 50-year-old woman accidentally hit her right eye with a metal tube. The next day she first noticed symptoms of this retinal detachment, which was caused by this usually long and narrow horseshoe tear. Note the rolled edges on each side of the tear and the long blood vessel running down the length of the flap. This illustrates the rule that when traction is exerted on the retina, the retinal blood vessels have a relative resistance to tearing and are the last areas to rupture.
Condition/keywords: retinal vessel, rolled edges of retina
-
 Acute Posterior Vitreous Detachment
Acute Posterior Vitreous Detachment
Nov 9 2012 by Norman Byer
This large and complicated retinal tear in a 51-year-old man resulted from an acute posterior vitreous detachment which concentrated its tractional forces around this area of lattice degeneration. Because of the powerful traction, there is an additional central tear splitting the large retinal flap and almost severing one of its arms. The traction was strong enough to completely rupture the blood vessel just to the left of the flap. Marking the ruptured peripheral end of the blood vessel is a yellow depigmented thrombus.
Condition/keywords: acute posterior vitreous detachment, depigmented thrombus, lattice degeneration, retinal tear, tractional retinal detachment
-
 Dialysis of Retina in Upper Nasal Quadrant
Dialysis of Retina in Upper Nasal Quadrant
Nov 9 2012 by Norman Byer
This 20-year-old wrestler sustained a sharp powerful blow to his right eye from his opponent’s thumb. One hour later he saw hundreds of black specs in his vision and was found to have this dialysis of his retina in the upper nasal quadrant. Note the triangular piece of retina in the center that remained attached to the ora serrata causing the retinal flap to resemble a man’s flared shirt collar.
Condition/keywords: retinal dialysis, retinal tear, upper nasal quadrant
-
 Congenital Meridional
Congenital Meridional
Nov 9 2012 by Norman Byer
This is the same case as seen in the previous photograph but showing an area just below the lower end of the dialysis. It shows a congenital meridional fold at the 2 o’clock meridian with a retinal break at the posterior end possibly caused by the direct injury described previously.
Condition/keywords: meridional fold, ora serrata, retinal break
-
 Inactive Toxoplasmosis
Inactive Toxoplasmosis
Nov 9 2012 by Norman Byer
This 28-year-old man had inactive toxoplasmosis and presented with acute symptoms caused by this tractional retinal tear adjacent to a retinochorodial scar. He also had an acute posterior vitreous detachment which had torn this retinal operculum completely free. The next slide shows the same lesion. Note the early rolled edge on the left side of the tear.
Condition/keywords: acute posterior vitreous detachment, inactive toxoplasmosis, operculum, rolled edges of retina, tractional retinal tear
-
 Inactive Toxoplasmosis
Inactive Toxoplasmosis
Nov 9 2012 by Norman Byer
This is the same case as in the previous photograph showing the very large free operculum torn from the retina.
Condition/keywords: acute posterior vitreous detachment, free operculum, inactive toxoplasmosis, tractional retinal tear
-
 Pars Planitis - Peripheral Uveitis
Pars Planitis - Peripheral Uveitis
Nov 9 2012 by Norman Byer
This 25-year-old man had pars planitis, peripheral uveitis bilaterally. In this eye it produced a small tractional oval tear of the retina and an inferior retinal detachment. The typical creamy yellow exudates of pars planitis can be seen in the lower right very close to the ora serrata.
Condition/keywords: creamy yellow exudates, inferior retinal detachment, pars planitis, peripheral uveitis, tractional retinal tear
-
 Lattice Lesion
Lattice Lesion
Nov 9 2012 by Norman Byer
This 55-year-old woman had had a cataract extraction five years earlier and also cryotherapy of some but not all of her lattice lesions. She was found to have this large retinal flap in the periphery near an area where cryotherapy had been applied. The next slide pair shows a different view of this lesion.
Condition/keywords: cataract extraction, cryotherapy, lattice lesion, retinal flap
-
 Retinal Break at Site of Lattice Degeneration with Scleral Indentation
Retinal Break at Site of Lattice Degeneration with Scleral Indentation
Nov 9 2012 by Norman Byer
This is the same case as the previous photograph. With scleral indentation slightly more posterior, the flap is seen to be associated with a large retinal tear. This is a tractional tear and it is possible that in this case the cryotherapy itself may have increased the vitreoretinal traction at this site and in this way led to this new tear. The age of the tear is unknown because it was asymptomatic, and even though the eye is aphakic the tear has not caused a clinical retinal detachment.
Condition/keywords: retinal flap, scleral indentation, tractional retinal tear, vitreoretinal traction
-
 Subclinical Retinal Detachment
Subclinical Retinal Detachment
Nov 9 2012 by Norman Byer
This 50-year-old man was treated with cryotherapy for two tiny non tractional round holes which had produced a small subclinical retinal detachment at 7:00 o’clock in this eye. Two years later he was seen with this large horseshoe tractional tear just anterior to the treated area and we must assume that it was a complication of that treatment.
Condition/keywords: cryotherapy, non-tractional holes, tractional retinal tear
-
 Senile Retinoschisis
Senile Retinoschisis
Nov 9 2012 by Norman Byer
This 48-year-old woman has senile retinoschisis involving the most common location, the lower temporal quadrant. The lesion shown here illustrates one of the two clinical features which are most often responsible for attracting the attention of the examiner to such lesions, namely the multitude of yellow flecks lying on the inner surface of the inner layer. The nature of these flecks is not known, but it seems clear that they do not originate in the schisis cavity for they do not represent remnants of ruptured Miller’s fibers. In this photograph you can easily detect the fluid space which separates the inner and outer retinal layers.
Condition/keywords: lower temporal quadrant, senile retinoschisis, yellow flecks
-
 Senile Retinoschisis
Senile Retinoschisis
Nov 9 2012 by Norman Byer
This is the same case as seen in the previous photograph but is a different view with the scleral indentation moved more anterior. The retinoschisis is seen to be very peripheral coming at least grossly right up to the ora serrata. Please notice how clear a view one can get of the ora serrata and pars plana using indirect ophthalmoscopy with scleral indentation.
Condition/keywords: ora serrata, retinoschisis, scleral indentation
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This 65-year-old woman illustrates the other most common clinical clue that leads to the discovery of retinoschisis namely the presence of one or more white occluded blood vessels in the inner layer of the lesion.
Condition/keywords: retinoschisis, white occluded blood vessels
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
These whitish spots in the inner layer are an uncommon finding in retinoschisis. When this highly elevated lesion was first discovered in this 45- year-old woman, it extended to within 25 degrees of the macula. Eleven years later it was exactly the same; although, the eye had received no treatment. This illustrates the predominant characteristic of this disease namely that it is usually non progressive.
Condition/keywords: retinoschisis, white spots in inner layer
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This 53-year-old man has retinoschisis involving the upper temporal quadrant but with no visible yellow dots or white lines to make it obvious. However, with scleral indentation you can see a large convex area showing the so-called white with pressure phenomenon. This area corresponds exactly to the area being indented and therefore must arise either from the outer layer of the retina or from some structure deep to it. White with pressure is an interesting optical phenomenon of uncertain origin but of no definite diagnostic or prognostic significance.
Condition/keywords: retinoschisis, scleral indentation, white with pressure
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This 57-year-old man has three large breaks in the outer layer of his retinoschisis. Note the interesting bridges separating the breaks and also note that the intact inner layer is only slightly elevated above the outer layer. This eye has not been treated and has remained essentially the same for eight years. Please note the yellow dots on the surface of the inner layer and the blood vessels running through this layer.
Condition/keywords: intact inner layer, outer layer breaks, retinoschisis, yellow dots
-
 Senile Retinoschisis
Senile Retinoschisis
Nov 9 2012 by Norman Byer
Senile retinoschisis in a 40-year-old woman showing a very large outer layer hole and a smaller one just above it. The inner layer is intact as shown by the blood vessels running through this layer. Note the prominent, sharp, yellow border at the upper and left edges of the large hole. This is caused by an inward rolling of the border of the outer layer and tends to be much more common along the posterior edges of holes in the outer layer in retinoschisis. This is an example of a schisis detachment with onset before age 40. It extends posteriorly to a .2½ disc diameters from the macula and has remained essentially "arrested" at this location for more than 17 years. A similar symmetrical "schisis-detachment" is present in the fellow eye.
Condition/keywords: intact inner layer, outer layer hole, schisis detachment, senile retinoschisis
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This 69-year-old woman has retinoschisis involving the inferior temporal quadrant. There are two outer layer holes each with a rolled posterior border. This lesion has looked exactly the same for 17 years with no treatment.
Condition/keywords: outer layer hole, retinoschisis, rolled edges of retina
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
The next three photographs are all of the same lesion in a 51 year-old man with retinoschisis. This photograph was taken without scleral indentation and shows the posterior border of this highly elevated fluid-filled lesion on the left half of the slide. It is unusual for the posterior edge to be demarcated this distinctly.
Condition/keywords: elevated, fluid-filled, retinoschisis
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This is a different view of the previous case taken with scleral indentation. There is a very large outer layer hole on the left side of the photograph with prominent yellow rolled posterior borders and a small yellow nubbin in the middle, which is probably the remnant of a former bridge between two smaller holes. This case has not been treated and has not progressed during four year’s observation. In fact, it has gotten measurably smaller in extent.
Condition/keywords: intact inner layer, outer layer hole, retinoschisis, rolled edges of retina, scleral indentation
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This is the same case as the previous two examples. The large outer layer hole of the previous photograph has led to a localized detachment of the outer layer. In this photograph, the camera is focused on the inner surface of the outer layer in order to show its irregular fur-like contour. Note also the tiny yellow dots of the inner layer superimposed on the dark indentation shadow. There is a fluid-filled space not only to the right but also to the left of the convex yellow line of the outer retinal layer indicating that the outer layer is elevated.
Condition/keywords: elevated outer layer, intact inner layer, localized detachment of outer layer, outer layer hole, retinoschisis, yellow dots
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This 60-year-old woman has had this outer layer hole in her retinoschisis for six years without much change in appearance. Note the prominent yellow line extending down from the lower end of the hole. This line identifies the outer layer and probably represents a small fold in this layer. The appearing of such a line and changes in it probably signal the beginning of a detachment of the outer layer in retinoschisis.
Condition/keywords: fold in outer layer of retinoschisis, intact inner layer, localized detachment of outer layer, outer layer hole, retinoschisis
-
 Retinoschisis
Retinoschisis
Nov 9 2012 by Norman Byer
This 51-year-old woman has retinoschisis with a large outer layer hole which has a white posterior rolled border. The left side of the posterior border of this hole can be seen to lie quite close to the inner layer showing that the outer layer is detached. This, therefore, is actually a combined schisis detachment which may safely be observed without treatment. This is an asymptomatic process, and the detachment of the outer layer is almost always localized and self limited.
Condition/keywords: intact inner layer, localized detachment of outer layer, outer layer hole, retinoschisis, rolled edges of retina, schisis detachment, white posterior
-
 Retinoschisis Detachment
Retinoschisis Detachment
Nov 9 2012 by Norman Byer
Combined retinoschisis detachment, so-called schisis detachment, in a 47-year-old woman. The large outer layer hole in the center has a posterior yellow border which represents the position of the outer layer. Please observe superior to the hole the dark convexity of the scleral indentation. Just below the hole at the middle of the slide and going to the left the yellow zone comes to lie right against the inner layer and a fluid filled cavity lies deep to the outer layer. At this point, therefore, there is a true neurosensory detachment of the retina. On the right side of the hole, the yellow line slants up and to the right and lies close to the pigment epithelium. On the right side of the photograph, the original schisis cavity can be seen separating the yellow line of the outer layer above from the inner retinal layer below. The mechanism of this detachment is that some of the fluid from the schisis cavity passes through the outer layer hole and detaches the outer layer. This lesion has not been treated and has remained exactly the same for 13 years. A similar symmetrical "schisis-detachment" is present in the fellow eye.
Condition/keywords: neurosensory detachment of retina, outer layer hole, pigment epithelium, retinoschisis, schisis detachment, scleral indentation
-
 Retinal Schisis Detachment
Retinal Schisis Detachment
Nov 9 2012 by Norman Byer
This 57-year-old man has a combined retinal schisis detachment caused by an outer layer hole in the upper right. On the right half of this photograph, the outer layer is detached and represented by the prominent yellow line which is lying against the inner layer. On the left half the inner layer appears very thin and the schisis cavity lies just behind it as it was originally. This, therefore, represents a localized detachment of the outer layer and thus a true secondary retinal detachment. The reason these cases remain localized and nonprogressive is that the only fluid available to the subretinal space is that which is contained within the schisis cavity. Furthermore, this fluid tends to be quite viscous and is not readily passed through the retinal breaks. A clinical symptomatic progressive retinal detachment cannot occur unless the retinal schisis cavity is very large or a break occurs in the inner layer also.
Condition/keywords: intact inner layer, localized detachment of outer layer, outer layer hole, retinal schisis detachment, retinoschisis, secondary retinal detachment
-
 Retinalschisis
Retinalschisis
Nov 9 2012 by Norman Byer
This 43-year-old woman had the small area of retinalschisis and associated small localized retinal detachment resulting from breaks in both retinal layers when she was first examined. This eye was asymptomatic and has remained exactly the same during two years of observation without treatment. In this picture, the outer layer break is demarcated by the yellow line. The inner layer is seen intact over this hole but has itself two small holes in the upper part of the photograph. Thus, it is evident that even retinoschisis with double layer holes does not necessarily progress to a clinical retinal detachment. The viscous nature of the fluid in the retinoschisis cavity is probably a contributing factor in this non progressive tendency.
Condition/keywords: inner layer holes, outer layer hole, retinoschisis
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
This is the same lesion as seen in the previous photograph but with the scleral indentation placed more anterior. In this view, one can look through both the inner and outer layer holes at the same time directly into the subretinal space. This is only a subclinical detachment which did not progress. True clinical progressive retinal detachments as a complication of retinoschisis probably do not occur in more than 1 of every 1,000 cases of senile retinoschisis.
Condition/keywords: inner layer holes, outer layer hole, retinoschisis, scleral indentation, subclinical detachment, subretinal space
-
 Yellow Globular Lesion
Yellow Globular Lesion
Nov 9 2012 by Norman Byer
This glistening yellow globular lesion is a so-called pearl of the ora serrata in a 45-year-old man. Notice location in the tooth of the ora, which is a characteristic of this lesion. Histologically pearls are drusen-like structures which form on the inner side of Bruch’s membrane beneath the pigment epithelium. They are seen in about 20% of eyes and are often bilaterally symmetrical. They have no clinical significance but are valuable as landmarks.
Condition/keywords: Bruch's membrane, drusen-like, ora serrata
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
The next three photographs are of the same lesion in a 26-year-old man and demonstrate the value of scleral indentation. This view without indentation shows only a tiny pigmented and atrophic spot in the fundus.
Condition/keywords: atrophic spot, pigmented lesion, scleral indentation
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
This is the same lesion as in the previous photograph. As scleral indentation begins, we see that the former tiny spot is actually the center of a larger whiter zone of uncertain etiology.
Condition/keywords: atrophic spot, scleral indentation, white retinal lesion
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
This is the same lesion as in the two previous photographs. With the scleral indentation placed more anterior, this white area is made to lie on the crest of the bulge where it can now be studied in profile. It projects above the retina and has sloping margins. The exact nature of this lesion is not known. This illustrates how the use of scleral indentation with indirect ophthalmoscopy can markedly change the appearance of retinal abnormalities and can bring to light many details not otherwise visible.
Condition/keywords: elevated retinal lesion, scleral indentation, white retinal lesion
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
The next two photographs are of the same lesion in a 43-year-old man. This view shows a small whitish lesion that appears to be attached to the retina at the crest of the scleral indentation.
Condition/keywords: elevated retinal lesion, scleral indentation, white retinal lesion
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
This is the same lesion as in the previous photograph. With the scleral indentation placed slightly more anterior, it is now apparent that the lesion lies almost entirely in the peripheral vitreous with only a tiny counterpart on the surface of the retina. Without scleral indentation, the exact location of this lesion would not have been known.
Condition/keywords: scleral indentation, vitreous lesion, white retinal lesion
-
 Meridional Fold
Meridional Fold
Nov 9 2012 by Norman Byer
The next two photographs are of the same lesion in a 28-year-old woman. This view shows a sloping retinal mound with a radial retinal fold in the center. This is not a typical meridional fold for it stops short of the ora serrata and there is no dentate process. The upper temporal ora serrata and pars plana are well shown and peripheral cystoid degeneration is present posterior to the ora.
Condition/keywords: ora serrata, pars plana, peripheral cystoid degeneration, radial retinal fold, sloping retinal mound
-
 Meridional Fold
Meridional Fold
Nov 9 2012 by Norman Byer
This is the same lesion as in the previous photograph. With the scleral indentation placed more posterior, we now can see that the fold ends over a small collection of subretinal fluid and that there is a very tiny retinal hole just below the posterior end of the retinal fold.
Condition/keywords: peripheral cystoid degeneration, retinal fold, retinal hole, scleral indentation, subretinal fluid
-
 White with Pressure Phenomenon
White with Pressure Phenomenon
Nov 9 2012 by Norman Byer
This photograph shows a rather typical example of the white with pressure phenomenon. It may take many forms but usually has a geographic configuration with irregular borders which may be rounded or angular. Its cause is unknown but it is a very common finding in the fundus. It is important to know that it does not indicate the presence of any disease of the retina. Over a period of time, it may disappear completely or it may change its configuration or location. Other examples of this phenomenon are shown in slide pairs 81 and 103.
Condition/keywords: geographic configuration, irregular borders, white retinal lesion, white with pressure
-
 Pseudo Retinal Break
Pseudo Retinal Break
Nov 9 2012 by Norman Byer
The next three photographs will illustrate retinal conditions that can easily be mistaken for retinal breaks. For a fourth example of a pseudo retinal break, see slide pair 35. It is important to distinguish these conditions from true retinal breaks. This 49-year-old man was found to have this crescent shaped reddish lesion with a sharp yellow posterior border but without any visible elevated retinal flap. The two blood vessels which traversed this lesion in the presence of a flat retina proved that the retina is intact. This confusing appearance is caused by the presence of white with pressure both behind and in front of the reddish area causing it to resemble a retinal break.
Condition/keywords: pseudo retinal break, reddish lesion, retinal flap, traversing retinal vessels, white with pressure
-
 Pseudo Retinal Break
Pseudo Retinal Break
Nov 9 2012 by Norman Byer
This large reddish area in the nasal periphery of this left eye is actually an enclosed ora bay. For other examples of this, see slide pair 5 and 6. This developmental abnormality could easily be confused with a retinal break. A very unusual feature of this photograph is the presence of a tiny true retinal break at the far right end of the enclosed ora bay and lying just to the left of the yellow zone in the middle of the photograph
Condition/keywords: enclosed ora bay, pseudo retinal break, reddish areas
-
 Pseudo Retinal Break
Pseudo Retinal Break
Nov 9 2012 by Norman Byer
This 23-year-old man presented with a fresh retinal detachment in a highly myopic eye and this very unusual retinal appearance. You can see two reddish areas with fairly distinct borders which at first make us think of retinal breaks. However, the left area has two tiny vessels visible in it, and the right area shows visible translucent retinal tissue extending across it. This patient has extensive areas of paving stone degeneration. Usually, such lesions present a barrier to a detaching retina and areas of paving stone usually remain attached. However, in this photograph we can see two paving stone lesions, and the detachment has extended right through them peeling them off from the underlying pigment epithelium. The two reddish areas, therefore, represent the very thin retina which previously constituted part of two paving stone lesions. The yellow atrophic areas which are visible deep to the detached retina represent the deeper parts of the same two original paving stone lesions.
Condition/keywords: myopic eye, pigment epithelium, reddish lesion, yellow atrophic area
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
On the crest of this indentation, one can see a small fragment of residual vitreous blood lying close to the retinal surface. The center is becoming typically white as the blood is becoming depigmented.
Condition/keywords: depigmented vitreous blood, scleral indentation, vitreous blood
-
 Double Elevated White Lesion
Double Elevated White Lesion
Nov 9 2012 by Norman Byer
This interesting double elevated white lesion in a 33-year-old woman is well seen in sharp relief on the crest of the scleral indentation. This exact nature of this lesion is not known.
Condition/keywords: scleral indentation, white retinal lesion
-
 Retained Green Mersilene Suture
Retained Green Mersilene Suture
Nov 9 2012 by Norman Byer
This 62-year-old dentist had had three retinal operations including an encircling polyethylene tube with silicone implant in 1962 and the removal of these elements 11 years later. This slide shows a retained green Mersilene suture which had been placed in the sclera more than 19 years before. It had slowly eroded inward and become subretinal. The retina is attached and the vision is 20/70.
Condition/keywords: retained green mersilene suture, subretinal
-
 Without Scleral Indentation
Without Scleral Indentation
Nov 9 2012 by Norman Byer
This 54-year-old woman presented with a history of sudden light flashes and black floaters for five days. Without scleral indentation, her right eye showed this lesion at 10:30 just 4 disc diameters from the macular. This slide is the first of a series of six photographs showing the lesion in different stages.
Condition/keywords: black floaters, preretinal hemorrhage, without scleral indentation
-
 Scleral Indentation
Scleral Indentation
Nov 9 2012 by Norman Byer
This is the same lesion with scleral indentation. You can see the small discrete preretinal hemorrhage and the sharply circumscribed area of elevated retina with subretinal fluid beneath it. No retinal break is visible, but the posterior vitreous is detached and exerting traction at this site. The area was surrounded with argon laser treatment the same day as the initial examination.
Condition/keywords: posterior vitreous detachment, preretinal hemorrhage, scleral indentation, subretinal fluid, vitreous traction
-
 Laser Photocoagulation
Laser Photocoagulation
Nov 9 2012 by Norman Byer
This shows the same lesion four days after laser photo coagulation. The new hemorrhages seen in this photograph did not occur during the photocoagulation but developed within the next four days.
Condition/keywords: argon photocoagulation, laser photocoagulation, preretinal hemorrhage
-
 Laser Photocoagulation
Laser Photocoagulation
Nov 9 2012 by Norman Byer
This shows the same lesion 11 days following laser photocoagulation. Still more new hemorrhages can now be seen, and the retinal tissue in the center of the lesion is being visibly pulled forward. If you look carefully, you can see the sharp lower edge of a developing tractional horseshoe tear.
Condition/keywords: laser photocoagulation, retinal tissue, vitreous traction
-
 Laser Photocoagulation
Laser Photocoagulation
Nov 9 2012 by Norman Byer
This is the same lesion 18 days following photocoagulation. The continuing vitreoretinal traction has now torn the retinal flap completely away from the retina and the resulting free operculum may be seen out of focus in the lower part of the photograph. The retinal tear is now easily visible with only a tiny remaining nubbin of the original flap seen above with a small hemorrhage.
Condition/keywords: free operculum, laser photocoagulation, retinal tear, vitreoretinal traction
-
 Tractional Retinal Tear
Tractional Retinal Tear
Nov 9 2012 by Norman Byer
This is the same lesion and shows the free operculum in better focus. This is an unusual location for a tractional retinal tear, and the increased mobility of the detached vitreous in the posterior part of the eye may have been a factor leading to the complete rupture of this retinal flap.
Condition/keywords: detached vitreous, free operculum, tractional retinal tear
-
 Cyst of the Pars Plana
Cyst of the Pars Plana
Nov 9 2012 by Norman Byer
This is a cyst of the pars plana located just anterior to the ora serrata in the lower temporal quadrant. It illustrates how far anterior one may visualize the fundus with indirect ophthalmoscopy and scleral indentation. Pars plana cysts are common lesions of no particular clinical significance.
Condition/keywords: cyst of the pars plana, lower temporal quadrant, ora serrata, scleral indentation
-
 Elevated Cystic Area
Elevated Cystic Area
Nov 9 2012 by Norman Byer
This is the eye of a 53-year-old woman with a small elevated cystic area of the peripheral retina at the posterior end of a meridional fold.
Condition/keywords: meridional fold, ora serrata, peripheral retina, small elevated cystic area
-
 Retinal Lesion
Retinal Lesion
Nov 9 2012 by Norman Byer
This 30-year-old man sustained a severe blow to his brow region which resulted in a variety of injuries including hyphema and vitreous and retinal hemorrhages. This photograph shows a retinal lesion, which is either a tiny area of elevated full thickness retina or a traumatic retinal cyst.
Condition/keywords: elevated retinal lesion, retinal hemorrhage, traumatic retinal cyst
-
 Retinal Detachment
Retinal Detachment
Nov 9 2012 by Norman Byer
This eye of a 25-year-old man has a retinal detachment of about six year’s duration. This photograph shows an intraretinal cyst, which is a secondary result of the longstanding detachment.
Condition/keywords: intraretinal cyst
-
 Retinal Detachment
Retinal Detachment
Nov 9 2012 by Norman Byer
This 18-year-old girl gave the history of having been hit in this eye three years before with a fist and of having retinal surgery nine months previously, which was temporarily successful. When the photograph was taken, she had a total left retinal detachment with a small nasal dialysis which had not been treated. She also had two prominent intraretinal cysts, one of which is shown here. The retina promptly reattached following further surgery and the next slide shows an interesting change in this cyst.
Condition/keywords: intraretinal cyst, small nasal dialysis
-
 Retinal Detachment
Retinal Detachment
Nov 9 2012 by Norman Byer
This is the same lesion as in the previous photograph shown 13 days after surgery. Not only is the retina reattached, but the cyst has now completely disappeared even though no treatment of any kind was applied in the vicinity of the cyst. Long detached retinas tend to develop intraretinal cysts, and these tend to disappear following reattachment of the retina even without direct treatment to the cysts.
Condition/keywords: intraretinal cyst, re-attached retinal detachment (RRD)
A project from the American Society of Retina Specialists