Search results (45 results)
-
 Acute Syphilitic Posterior Placoid Chorioretinitis
Acute Syphilitic Posterior Placoid Chorioretinitis
Nov 1 2025 by Julián Villarreal, MD
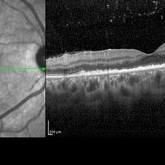
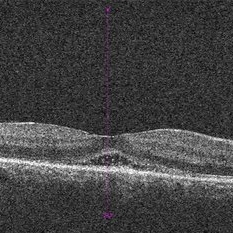
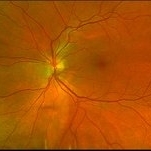
A 48 year old male presented with Acute syphilitic posterior placoid chorioretinitis (ASPPC) a large, roundish, yellowish, placoid lesion occurring at level of the retinal pigment epithelium (RPE) at the macular/paramacular area. Further testing showed a reactive VDRL and a positive FTA-ABS.
Photographer: Julián Villarreal MD
Imaging device: Mirante
Condition/keywords: Preretinal precipitates
-
 Posterior Placoid Chorioretinitis
Posterior Placoid Chorioretinitis
Mar 9 2025 by Oscar Francisco Miranda, MD
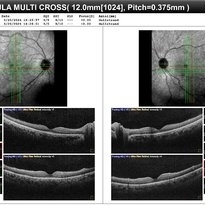
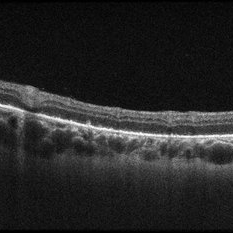
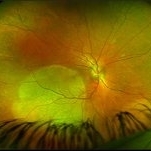
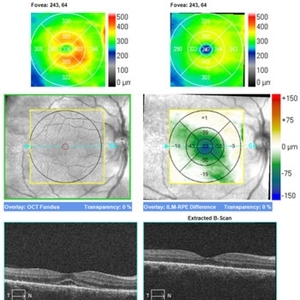
A 36-year-old male with bilateral visual loss of 3 months' duration, with no relevant medical history on inquiry. A round-shaped lesion with well-defined borders and a yellowish-white color is observed in the macula of both eyes, accompanied by vitreous cellularity. The macular OCT shows a dentate RPE. The VDRL, FTA-ABS, and HIV tests were positive.
Photographer: Oscar Francisco Miranda-Gómez
Imaging device: Heidelberg Spectralis
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, OCT, Ocular syphilis
-
 Posterior Placoid Chorioretinitis
Posterior Placoid Chorioretinitis
Mar 9 2025 by Oscar Francisco Miranda, MD
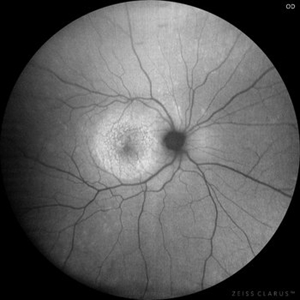
A 36-year-old male with bilateral visual loss of 3 months' duration, with no relevant medical history on inquiry. A round-shaped lesion with well-defined borders and a yellowish-white color is observed in the macula of both eyes, accompanied by vitreous cellularity. The macular OCT shows a dentate RPE. The VDRL, FTA-ABS, and HIV tests were positive.
Photographer: Oscar Francisco Miranda-Gómez
Imaging device: Autofluorescence Zeiss Clarus 700
Condition/keywords: acute posterior placoid chorioretinitis, Autofluorescence, ocular syphilis
-
 Posterior Placoid Chorioretinitis
Posterior Placoid Chorioretinitis
Mar 9 2025 by Oscar Francisco Miranda, MD
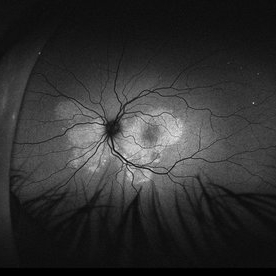
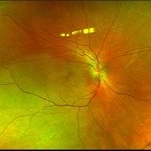
A 36-year-old male with bilateral visual loss of 3 months' duration, with no relevant medical history on inquiry. A round-shaped lesion with well-defined borders and a yellowish-white color is observed in the macula of both eyes, accompanied by vitreous cellularity. The macular OCT shows a dentate RPE. The VDRL, FTA-ABS, and HIV tests were positive.
Photographer: Oscar Francisco Miranda-Gómez
Imaging device: Zeiss Clarus 700
Condition/keywords: acute posterior placoid chorioretinitis, Ocular syphilis
-
 Acute Syphilitic Posterior Placoid Chorioretinitis
Acute Syphilitic Posterior Placoid Chorioretinitis
Oct 20 2024 by César Adrián Gómez Valdivia, MD
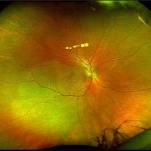
Fundus autofluorescence image of an acute syphilitic posterior placoid chorioretinitis found in a HIV positive 28 YO male patient with suspected neurosyphilis. A beautiful butterfly autofluorescence pattern can be appreciated.
Photographer: @eyemissu2
Imaging device: California ICG OPTOS
Condition/keywords: acute syphilitic posterior placoid chorioretinitis
-
 Acute Syphilitic Posterior Placoid Chorioretinitis
Acute Syphilitic Posterior Placoid Chorioretinitis
Oct 16 2024 by César Adrián Gómez Valdivia, MD
Fundus autofluorescence image of an acute syphilitic posterior placoid chorioretinitis found in a HIV positive 28 YO male patient with suspected neurosyphilis. A beautiful butterfly autofluorescence pattern can be appreciated.
Photographer: @eyemissu2
Imaging device: California ICG OPTOS
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, chorioretinitis, syphilis
-
 Syphilitic Posterior Uveitis
Syphilitic Posterior Uveitis
Mar 22 2024 by Anjana Mirajkar, MS Ophthalmology
An OCT image BE of 36 year old female showing RPE granularity and IS/OS irregularity in a case of syphilitic posterior placoid chorioretinitis
Photographer: Dr. Anjana Mirajkar -Retina Foundation, Ahmedabad
Condition/keywords: acute posterior placoid chorioretinitis, acute syphilitic posterior placoid chorioretinitis
-
 Syphilitic Posterior Uveitis
Syphilitic Posterior Uveitis
Mar 22 2024 by Anjana Mirajkar, MS Ophthalmology
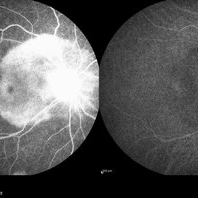
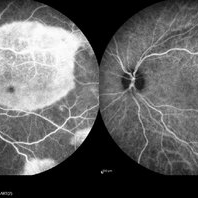
FA image of RE of a 36 year old female showing hyper-fluorescence (staining) from early to late phases of the angiogram in a case syphilitic posterior placoid chorioretinitis. ICG image depicts hypo-cyanence from early to late phases.
Photographer: Dr. Anjana Mirajkar -Retina Foundation, Ahmedabad
Imaging device: Heidelberg
Condition/keywords: acute syphilitic posterior placoid chorioretinitis
-
 Syphilitic Posterior Uveitis
Syphilitic Posterior Uveitis
Mar 22 2024 by Anjana Mirajkar, MS Ophthalmology
FA image of LE of a 36 year old female showing hyper-fluorescence (staining) from early to late phases of the angiogram in a case syphilitic posterior placoid chorioretinitis. ICG image depicts hypo-cyanence from early to late phases.
Photographer: Dr. Anjana Mirajkar -Retina Foundation, Ahmedabad
Condition/keywords: acute syphilitic posterior placoid chorioretinitis
-
 Syphilitic Posterior Uveitis
Syphilitic Posterior Uveitis
Mar 22 2024 by Anjana Mirajkar, MS Ophthalmology
A color photo image of RE of a 36 year old female showing hypopigmented lesions at the posterior pole(ground glass appearance) in a case of syphilitic posterior placoid chorioretinitis
Photographer: Dr. Anjana Mirajkar -Retina Foundation, Ahmedabad
Imaging device: Mirante-Nidek
Condition/keywords: posterior uveitis
-
 Syphilitic Posterior Uveitis
Syphilitic Posterior Uveitis
Mar 22 2024 by Anjana Mirajkar, MS Ophthalmology
A color photo image of LE of a 36 year old female showing hypopigmented lesions at the posterior pole(ground glass appearance) in a case of syphilitic posterior placoid chorioretinitis
Photographer: Dr. Anjana Mirajkar -Retina Foundation, Ahmedabad
Imaging device: Mirante-Nidek
Condition/keywords: syphilitic posterior uveitis
-
 Acute syphilitic posterior placoid chorioretinitis
Acute syphilitic posterior placoid chorioretinitis
Apr 24 2022 by Aniruddha K Agarwal, MD
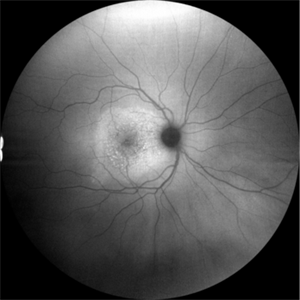
Green-light fundus autofluorescence (FAF) of the right eye from a 55-year-old man with risk factors for sexually trasnmitted diseases who presented to the retina clinic for a central scotoma. Funduscopy revealed a placoid lesion in the posterior pole. FAF highlights a hyperautofluorescent placoid lesion involving the macula with granular hyperfluorescence. The patient tested positive for syphilis and received intravenous penicillin treatment.
Photographer: Esther CIANCAS, MD, PhD, Gema CRESPO-RODRÍGUEZ, RN
Imaging device: Zeiss Clarus fundus camera
Condition/keywords: chorioretinitis, IUSG, syphilis, uveitis
-
 Acute Syphilitic Posterior Placoid Chorioretinitis (ASPPC)
Acute Syphilitic Posterior Placoid Chorioretinitis (ASPPC)
May 12 2021 by Joseph D Boss, MD
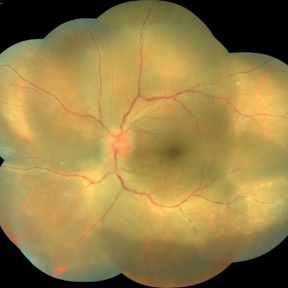
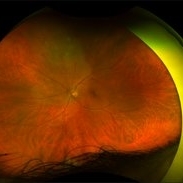
Ultra-widefield fundus photograph of a 36-year-old male with acute syphilitic posterior placoid chorioretinitis. Subsequent testing reviewed a positive RPR 1:256 and positive syphilis antibody.
Photographer: Joseph Boss, MD; Retina Specialists of Michigan
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, syphilitis uveitis
-
 Acute Syphilitic Posterior Placoid Chorioretinitis
Acute Syphilitic Posterior Placoid Chorioretinitis
May 4 2021 by RAFAEL REIS PEREIRA, MD
A 31-year-old patient with a complaint of photophobia and low visual acuity OD in the previous three weeks. BCVA was 20/60 and 20/20 The fundus examination revealed a placoid white lesion in the posterior pole and vitreous cells in the right eye. The left eye was unremarkable. Fluorescein angiography reveals hyperfluorescent plaque with distinctive “leopard spots” hypofluorescence.
Imaging device: Opto California
Condition/keywords: acute syphilitic posterior placoid chorioretinitis
-
 Acute Syphilitic Posterior Placoid Chorioretinitis with Papillitis
Acute Syphilitic Posterior Placoid Chorioretinitis with Papillitis
Mar 30 2021 by Tanya Jain
A 41-year-old homosexual male patient presented with placoid chorioretinitis and was diagnosed with acute syphilitic posterior placoid chorioretinitis, neurosyphilis and HIV disease. The patient was started with HAART and intravenous antibiotics.
Photographer: Tanya Jain
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, choroiditis, papillitis
-
 Palms of Patient with Placoid Lesions in Posterior Segment
Palms of Patient with Placoid Lesions in Posterior Segment
Dec 20 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), Plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, Pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery. There was trace vitreous cell OS, mild disc edema, and a large, granular placoid area nasally that appeared to be granulated. The OCT showed mild subfoveal fluid with nodular areas in the RPE and some overlying irregular architecture of the outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand (See Image), and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started). She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated. OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer.
Imaging device: Optos CA
Condition/keywords: acute syphilitic posterior placoid chorioretinitis
-
 Posterior Placoid Chorioretinopathy
Posterior Placoid Chorioretinopathy
Dec 19 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery. There was a trace vitreous cell OS with a large, granular placoid lesion nasally. The OCT (see above) shows mild subfoveal fluid with nodular areas in the RPE and some overlying irregular architecture of the outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand, and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started). She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated. OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer.
Imaging device: Zeiss Cirrus
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, syphilis
-
 Posterior Placoid Chorioretinopathy
Posterior Placoid Chorioretinopathy
Dec 19 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery. There was a trace vitreous cell OS with a large, granular placoid lesion nasally. The OCT via the lesion (see above) shows nodular areas in the RPE and some overlying disruption of EZ and outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand, and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started). She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated. OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer.
Imaging device: Zeiss Cirrus
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, syphilis
-
 Posterior Placoid Chorioretinopathy
Posterior Placoid Chorioretinopathy
Dec 19 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery. There was trace vitreous cell OS, mild disc edema, and a large, granular placoid area nasally that appeared to be granulated. The OCT showed mild subfoveal fluid with nodular areas in the RPE and some overlying irregular architecture of the outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand, and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started). She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated (See Image). OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer.
Photographer: Ashley Seiger
Imaging device: Optos CA
Condition/keywords: acute syphilitic posterior placoid chorioretinitis
-
 Posterior Placoid Chorioretinopathy
Posterior Placoid Chorioretinopathy
Dec 19 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery. There was trace vitreous cell OS, mild disc edema, and a large, granular placoid area nasally that appeared to be granulated. The OCT showed mild subfoveal fluid with nodular areas in the RPE and some overlying irregular architecture of the outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand, and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started). She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated (See Image). OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer.
Photographer: Ashley Seiger
Imaging device: Optos CA
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, syphilis
-
 Syphilis Placoid Initial Image OS
Syphilis Placoid Initial Image OS
Dec 19 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery. There was trace vitreous cell OS, mild disc edema, and a large, granular placoid area nasally that appeared to be granulated (See Image). The OCT showed mild subfoveal fluid with nodular areas in the RPE and some overlying irregular architecture of the outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand, and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started).... She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated. OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer.
Imaging device: Optos CA
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, syphilis
-
 Posterior Placoid Chorioretinopathy
Posterior Placoid Chorioretinopathy
Dec 19 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), Plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery, and two possible smaller spots SN (See Photo above). There was a trace vitreous cell OS with a large, granular placoid lesion nasally. The OCT showed mild subfoveal fluid with nodular areas in the RPE and some overlying irregular architecture of the outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand, and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started). She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated. OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer.
Imaging device: Optos CA
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, syphilis
-
 Posterior Placoid Chorioretinopathy
Posterior Placoid Chorioretinopathy
Dec 19 2020 by John S. King, MD
44-year-old white female seen over the weekend complaining of a "spot" in her vision centrally OD for three days. She was referred over by another eye doctor who was concerned about a possible retinal detachment vs ARN in that eye. Her past medical history includes adrenal insufficiency for which she takes a low dose of hydrocortisone, thyroxine (post thyroidectomy), plaquenil (inflammatory arthritis). She is divorced with one partner and denies any IVDU. Va 20/200 OD and 20/20 OS, IOP 12 OU, Pupils mydriatic post gtts (light desaturation OD). There was 1+ A/C cell OD, O/W unremarkable anterior segment OU; in the posterior segment OD there was 1+ vitritis with a diffusely swollen optic disc and a large yellowish placoid lesion in the macula with yellowish border and extended out past the arcades inferiorly, as well as another lesion smaller in the IN periphery. There was trace vitreous cell OS, mild disc edema, and a large, granular placoid area nasally that appeared to be granulated. The OCT showed mild subfoveal fluid with nodular areas in the RPE and some overlying irregular architecture of the outer retina. Syphilis was a concern at this point. She denied any hand or foot rash, and said that she was recently working on the house, and her hands were dried out. There did appear to be a rash on the hand, and later learned that she had a rash on the soles of her feet. She was sent to ED for a work-up and her syphilis IgG was positive and VDRL 1:128, and negative for HIV. She was started on a course IV Penicillin (40mg PO steroid two days after tx started). She has responded well. A few days after treatment her visual acuity has improved to 20/60 OD; there was no anterior segment inflammation OU, and decreased vitreous cell OU. Disc edema was improved. The large placoid lesion in the macula of the right eye was slightly enlarged, but more granular in appearance without a distinct yellowish border, and the smaller lesions SN had dissipated. OCT showed resolution of the subfoveal fluid and an improved appearance of the outer retina and RPE layer (See Image).
Imaging device: Zeiss Cirrus
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, syphilis
-
 Acute Syphilitic Posterior Placoid Chorioretinitis
Acute Syphilitic Posterior Placoid Chorioretinitis
Nov 22 2020 by Shawn Sell
58-year-old homeless male presenting with 2 weeks of bilateral eye redness and photosensitivity found to have panuveitis with a positive VDRL CSF and RPR titer of 1:512 with acute syphilitic posterior placoid chorioretinitis.
Photographer: Eastern Virginia Medical School
Imaging device: Optos
Condition/keywords: acute syphilitic posterior placoid chorioretinitis, neurosyphilis
-
 Acute Syphilitic Posterior Placoid Chorioretinitis
Acute Syphilitic Posterior Placoid Chorioretinitis
Nov 22 2020 by Shawn Sell
58-year-old homeless male presenting with 2 weeks of bilateral eye redness and photosensitivity found to have panuveitis with a positive VDRL CSF and RPR titer of 1:512 with acute syphilitic posterior placoid chorioretinitis.
Photographer: Eastern Virginia Medical School
Imaging device: Optos
Condition/keywords: acute syphilitic posterior placoid chorioretinitis
 Loading…
Loading…